With the tennis season in full swing, we look at one of the most common tennis injuries in more detail.
The shoulder enables a great range of motion and strength in the arm, but we ask a lot of this complex structure, particularly in tennis. Whether you are an elite competitor or a recreational, weekend player shoulder pain is one of the most common physical complaints faced by any tennis player.
The pain is mainly linked to overuse injuries related to the repetitive overhead activity of the muscles around the shoulder (particularly the rotator cuff) and those muscles that stabilise the shoulder blade (scapula).
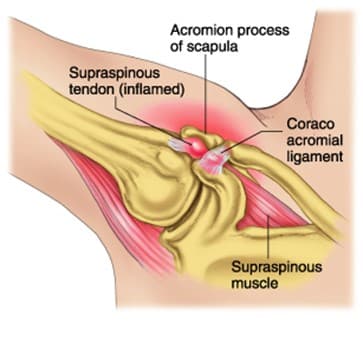
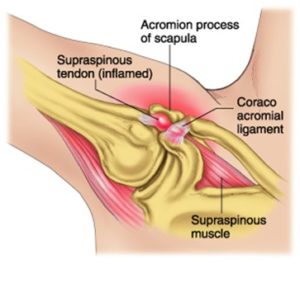
Shoulder impingement occurs when the top outer edge of your shoulder blade, called the acromion, rubs against, or pinches your rotator cuff tendons beneath it, causing pain, swelling and irritation – rotator cuff tendonitis. It can also affect the bursa too, which is a fluid-filled sack that sits between the bone and the rotator cuff tendons, this is known as subacromial bursitis.
Anatomy
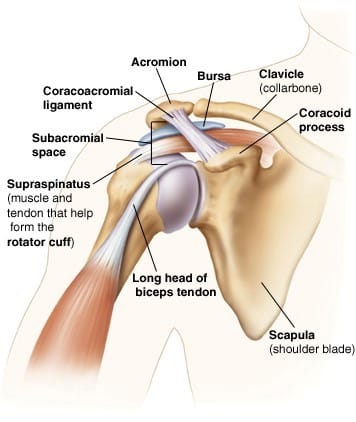
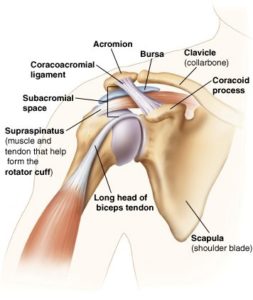
Your rotator cuff is a group of four muscles that originate on the shoulder blade and attach to your arm bone (humerus).
The role of the rotator cuff is to provide stability to the shoulder joint and help to produce movement such as lifting and rotating the arm.
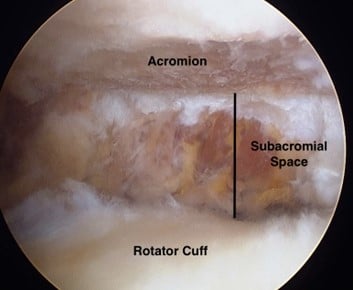
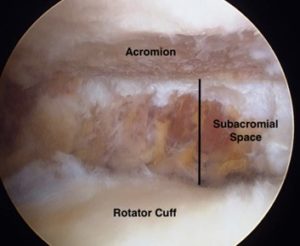
You use your rotator cuff to help raise your arm overhead and to rotate your arm towards and away from your body. The rotator cuff tendons sit in a small space between two bones in the shoulder (the acromion and the humerus), called the subacromial space. This arrangement makes the rotator cuff susceptible to being pinched or impinged between these bones, leading to what is called impingement syndrome.
Causes
In a tennis tournament, a player may perform hundreds of overhead activities such as serving, hitting high tops spin forehands, or hitting overhead smashes. These repeated, overhead movements can easily cause the rotator cuff to become injured or irritated. This irritation causes the tendon and bursa to swell, which reduces the amount of space around the rotator cuff, leading to rubbing against the acromion. Like a vicious cycle, the rubbing of the rotator cuff tendons results in more swelling, which further narrows the space below the acromion.
Another common cause of impingement is that the subacromial space becomes narrowed due to altered biomechanics of the shoulder – poor posture and muscle imbalances. If a player has some muscles in the shoulder that are stronger and some that are weaker, the shoulder joint can sit slightly forward in the socket. This causes the subacromial space to be narrowed which can then in turn make the tendons and bursa more likely to be irritated.
In some cases, bone spurs can develop on the acromion bone, these can contribute to impingement by causing the space where the rotator cuff sits to be even more narrowed. This is generally only seen in older players.
Risk Management
Tennis players can reduce their risk of injury in several ways:
- Avoid things that make the pain worse – Relative rest and activity modification. Reduce the amount of training and intensity.
- Review and correct technique of groundstrokes and serve.
- Address any posture and biomechanical dysfunctions of the shoulder and the wider kinetic chain.
- Strengthening exercises to increase shoulder blade (scapula) stabilisation, optimise rotator cuff strength, and specifically work on strength in the outer and inner ranges of movement of the shoulder.
- Improve core stability and lower limb strength.
- Do not stop moving your arm completely – try to carry on with your normal daily activities as much as possible so your shoulder does not become weak or stiff. It’s usually best to avoid using a sling.
- Ensure you are using the correct equipment especially the most appropriate tennis racquet grip size, weight, and string tension.
Make sure that you consult your coach and physio or specialist, who can give you guidance on the above.
Symptoms
Shoulder impingement can start suddenly or come on gradually. It is a condition that usually affects middle-aged players and high-performance players who are playing very regularly. The pain is worse with overhead activities such as serving, hitting high tops spin forehands, or hitting overhead smashes. There may be an aching pain after play.
Symptoms include:
- pain in the top and outer side of your shoulder
- pain that’s worse when you lift your arm, especially when you lift it above your head
- pain or aching at night, which can affect your sleep
- weakness in your arm
Symptoms can vary considerably depending on the exact cause and the severity of the condition. It is vital that you are seen by a specialist in order to get a quick and accurate diagnosis.
Your specialist at London Bridge Orthopaedics will assess your shoulder and send you for any additional diagnostic tests, to ensure you are treated timely and appropriately and to make sure you get back to playing the sport that you love!
Treatment
Medication
Oral anti-inflammatory medications — such as aspirin, naproxen, or ibuprofen, remain the most common treatment for impingement syndrome.
The medicines are usually given for six to eight weeks since it often takes that long to fully treat the problem. You should do this under the care of a doctor.
Physiotherapy
In the majority of cases, impingement syndrome can be treated conservatively with Physiotherapy. At London Bridge Orthopaedics we have excellent relationships with some of the best physiotherapists in London, and your consultant will refer you to someone they feel will be most appropriate for you
Injection
A steroid injection into your shoulder can help relieve pain if rest and exercises on their own do not help, or if the pain is preventing you from engaging in physiotherapy. This will help reduce the pain and inflammation and provide a window of opportunity for you to continue with your physio rehab. It is advised that you restart your physiotherapy two weeks after injection to gain the full benefit from this treatment option. Injections can be repeated if you have had an initial good outcome but need some further intervention to progress your rehab further. Steroid injections should be performed under ultrasound guidance to get the best possible outcome. This can all be arranged by your consultant at London Bridge Orthopaedics
Surgery
Surgery is considered if nonsurgical treatments don’t relieve your pain. One surgery called subacromial decompression or arthroscopic shoulder decompression removes part of the acromion to create more space for the rotator cuff. They may also remove part of the inflamed bursa. This procedure can usually be performed arthroscopically, which means through small cuts (incisions) in your shoulder.
Your surgeon may also treat other conditions present in the shoulder at the time of surgery. These can include:
- Arthritisbetween the clavicle (collarbone) and the acromion (acromioclavicular arthritis)
- Inflammation of the biceps tendon (biceps tendinitis)
- A partial rotator cuff tear
Following surgery, it is extremely important that you restart your physiotherapy-guided rehabilitation programme. This will be done slowly and gradually as you recover from your operation. Your physiotherapist will liaise closely with your surgeon to ensure you get the best possible outcomes.
It typically takes 2 to 4 months to achieve improved symptoms, but it may take up to a year to regain full shoulder function and strength.
At London Bridge Orthopaedics we have three shoulder consultants. Find out more.
If you would like to make a new patient appointment, please call now or you can fill out an appointment request form and we will contact you asap.